Authors: Daniel J Grint, Kevin Wing, Catherine Houlihan, Hamish P Gibbs, Stephen J W Evans, Elizabeth Williamson, Helen I McDonald, Krishnan Bhaskaran, David Evans, Alex J Walker, George Hickman, Emily Nightingale, Anna Schultze, Christopher T Rentsch, Chris Bates, Jonathan Cockburn, Helen J Curtis, Caroline E Morton, Sebastian Bacon, Simon Davy, Angel Y S Wong, Amir Mehrkar, Laurie Tomlinson, Ian J Douglas, Rohini Mathur, Brian MacKenna, Peter Ingelsby, Richard Croker, John Parry, Frank Hester, Sam Harper, Nicholas J DeVito, Will Hulme, John Tazare, Liam Smeeth, Ben Goldacre, Rosalind M Eggo
Published: July, 2022 in Clinical Infectious Diseases
Abstract
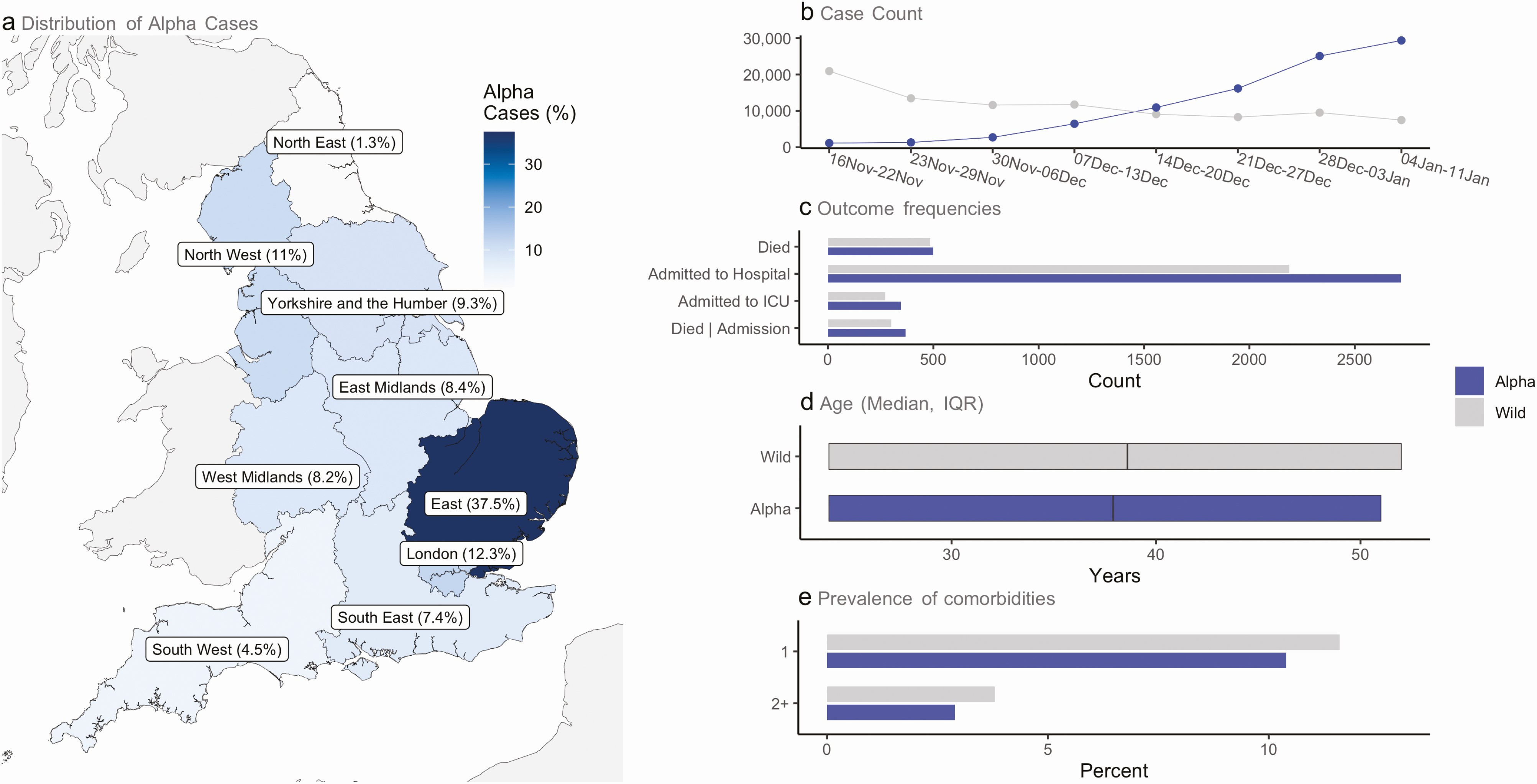
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) alpha variant (B.1.1.7) is associated with higher transmissibility than wild-type virus, becoming the dominant variant in England by January 2021. We aimed to describe the severity of the alpha variant in terms of the pathway of disease from testing positive to hospital admission and death.With the approval of NHS England, we linked individual-level data from primary care with SARS-CoV-2 community testing, hospital admission, and Office for National Statistics all-cause death data. We used testing data with S-gene target failure as a proxy for distinguishing alpha and wild-type cases, and stratified Cox proportional hazards regression to compare the relative severity of alpha cases with wild-type diagnosed from 16 November 2020 to 11 January 2021.Using data from 185 234 people who tested positive for SARS-CoV-2 in the community (alpha = 93 153; wild-type = 92 081), in fully adjusted analysis accounting for individual-level demographics and comorbidities as well as regional variation in infection incidence, we found alpha associated with 73% higher hazards of all-cause death (adjusted hazard ratio [aHR]: 1.73; 95% confidence interval [CI]: 1.41–2.13; P < .0001) and 62% higher hazards of hospital admission (1.62; 1.48–1.78; P < .0001) compared with wild-type virus. Among patients already admitted to the intensive care unit, the association between alpha and increased all-cause mortality was smaller and the CI included the null (aHR: 1.20; 95% CI: .74–1.95; P = .45).The SARS-CoV-2 alpha variant is associated with an increased risk of both hospitalization and mortality than wild-type virus.
Cite
@article{grint_severity_2022,
title = {Severity of Severe Acute Respiratory System Coronavirus 2 ({SARS}-{CoV}-2) Alpha Variant (B.1.1.7) in England},
volume = {75},
issn = {1058-4838},
url = {https://doi.org/10.1093/cid/ciab754},
doi = {10.1093/cid/ciab754},
abstract = {The severe acute respiratory syndrome coronavirus 2 ({SARS}-{CoV}-2) alpha variant (B.1.1.7) is associated with higher transmissibility than wild-type virus, becoming the dominant variant in England by January 2021. We aimed to describe the severity of the alpha variant in terms of the pathway of disease from testing positive to hospital admission and death.With the approval of {NHS} England, we linked individual-level data from primary care with {SARS}-{CoV}-2 community testing, hospital admission, and Office for National Statistics all-cause death data. We used testing data with S-gene target failure as a proxy for distinguishing alpha and wild-type cases, and stratified Cox proportional hazards regression to compare the relative severity of alpha cases with wild-type diagnosed from 16 November 2020 to 11 January 2021.Using data from 185 234 people who tested positive for {SARS}-{CoV}-2 in the community (alpha = 93 153; wild-type = 92 081), in fully adjusted analysis accounting for individual-level demographics and comorbidities as well as regional variation in infection incidence, we found alpha associated with 73\% higher hazards of all-cause death (adjusted hazard ratio [{aHR}]: 1.73; 95\% confidence interval [{CI}]: 1.41–2.13; P \< .0001) and 62\% higher hazards of hospital admission (1.62; 1.48–1.78; P \< .0001) compared with wild-type virus. Among patients already admitted to the intensive care unit, the association between alpha and increased all-cause mortality was smaller and the {CI} included the null ({aHR}: 1.20; 95\% {CI}: .74–1.95; P = .45).The {SARS}-{CoV}-2 alpha variant is associated with an increased risk of both hospitalization and mortality than wild-type virus.},
pages = {e1120--e1127},
number = {1},
journaltitle = {Clinical Infectious Diseases},
shortjournal = {Clinical Infectious Diseases},
author = {Grint, Daniel J and Wing, Kevin and Houlihan, Catherine and Gibbs, Hamish P and Evans, Stephen J W and Williamson, Elizabeth and {McDonald}, Helen I and Bhaskaran, Krishnan and Evans, David and Walker, Alex J and Hickman, George and Nightingale, Emily and Schultze, Anna and Rentsch, Christopher T and Bates, Chris and Cockburn, Jonathan and Curtis, Helen J and Morton, Caroline E and Bacon, Sebastian and Davy, Simon and Wong, Angel Y S and Mehrkar, Amir and Tomlinson, Laurie and Douglas, Ian J and Mathur, Rohini and {MacKenna}, Brian and Ingelsby, Peter and Croker, Richard and Parry, John and Hester, Frank and Harper, Sam and {DeVito}, Nicholas J and Hulme, Will and Tazare, John and Smeeth, Liam and Goldacre, Ben and Eggo, Rosalind M},
urldate = {2023-09-01},
date = {2022-07-01},
file = {Full Text PDF:/Users/hamishgibbs/Zotero/storage/67WWZ5LV/Grint et al. - 2022 - Severity of Severe Acute Respiratory System Corona.pdf:application/pdf;Snapshot:/Users/hamishgibbs/Zotero/storage/7RSSXDVD/6365124.html:text/html},
}